
REtina consultants OF PUERTO RICO
Procedures at RCPR
Retina Consultants of Puerto Rico, is one of the most accomplished retinal and macular care practices in the PR, offers the most sophisticated medical treatment and surgical management—and comprehensive patient care—of adult retinal diseases.

Main Procedures at RCPR
1. Focal Macular Laser
2. Panretinal Photocoagulation (PRP) Laser
3. Intravitreal Injections
4. Micro-Pulse Laser
5. Photodynamic Therapy ( PDT)
6. Pars Plana Vitrectomy
7. Scleral Buckle

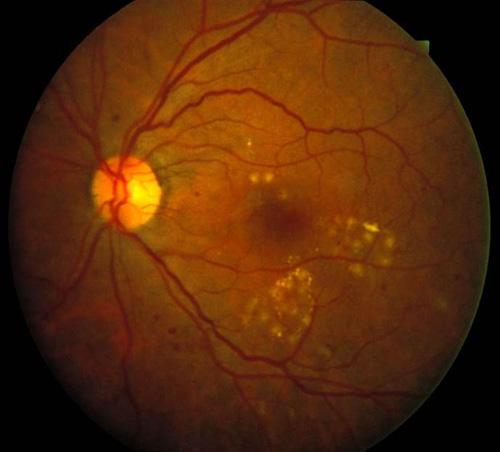
Focal Macular Laser
Focal laser is the direct application of thermal laser to leaking blood vessels to close them or to areas of retinal swelling (edema) to reduce it. This is done using topical anesthesia and a special contact lens used to image the retina. Indications for this type of laser are:
1. Diabetic Retinopathy with macular edema not involving the center of the macula.
2. Branch Retinal Vein Occlusion with macular edema
3. Retinal Arterial Macroaneuryms
4. Central Serous Retinopathy
5. Retinal/Choroidal Vascular tumors, such as Hemangiomas or Angiomas
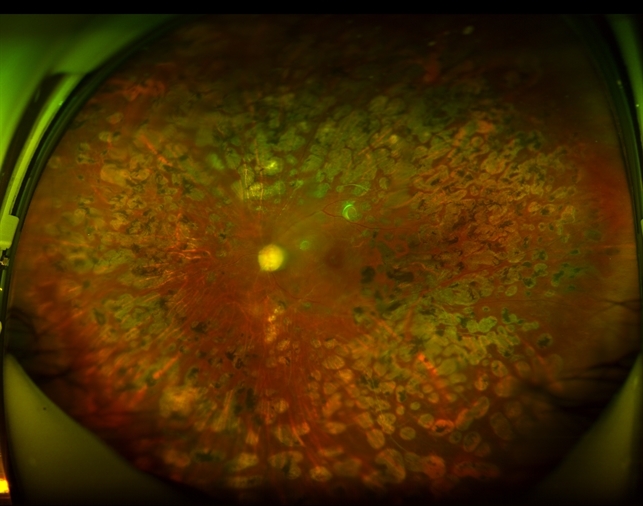
Panretinal Photocoagulation (PRP)
Laser Panretinal Photocoagulation (PRP) is a well-established, time-proven treatment for retinal diseases associated with retinal new blood vessels (neovascularization) such as Proliferative Diabetic Retinopathy and Retinal Vein Occlusions. This treatment is applied either with the use of a contact lens used to focus the laser rays or an Indirect laser system placed on the head of the Retinal surgeon. This laser is effective in preventing the progression of the disease, sealing the new blood vessels, and avoiding visually-devastating complications such as Retinal Detachments and Vitreous Hemorrhage.

Micropulse Laser Therapy (MPLT)
Micropulse Laser Therapy (MPLT) is a feature of the Iridex IQ577 laser we recently acquired. Conventional continuous thermal laser, as used for Diabetic Macular Edema (DME) causes actual damage to the RPE cells with potential collateral damage to adjacent cells near the fovea. MPLT uses technology to “chop” a continuous wave laser beam into multiple, repetitive microsecond pulses, allowing the retinal tissue to cool between pulses and thus reduce thermal damage. This new laser technology, while not a panacea on its own, has been shown to be useful for augmenting therapy effect for DME with intravitreal anti-VEGF agents while at the same time helping reduce the number of injections performed. MPLT can be applied directly over the fovea with no collateral damage. Other uses for MPLT are for refractory Central Serous Retinopathy and Retinal Vein Occlusions with macular edema.
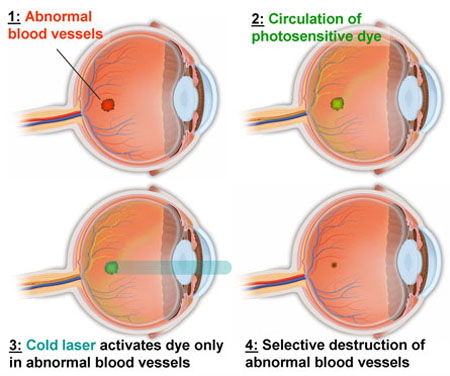
Ocular Photodynamic Therapy
Ocular Photodynamic Therapy is a treatment option used primarily for resistant Wet Age-Related Macular Degeneration, Polypoidal Choroidal Vaculopathy and for Choroidal tumors such as Choroidal Hemangiomas. This type of cold laser allows the abnormal blood vessels to close without causing heat damage to the overlying healthy retina. Benefits include potential improvement or stabilization of the retinal lesion, therefore decreasing the rate of visual loss. Photodynamic Therapy requires the injection of the drug Visudyne®.
You will receive a 10-minute intravenous (IV) infusion of Visudyne®. The dosage of medication is determined by each individual patient’s height and weight. Infusion-related problems include leaking of fluid at the infusion site that can lead to skin injury, back pain, and allergic sensitivity to the infused medication. An activating light (laser) will be shone in your eye 5 minutes after the infusion ends. This laser is a much lower energy than is used in conventional laser surgery and has no effect without the Visudyne® drug in the circulation. The liver rapidly eliminates Visudyne®. Therefore, you may notice that your stools are dark in color for a few days after treatment.
Only 1% -4% of patients have improved vision after Visudyne® Photodynamic Therapy treatment. The purpose of these treatments is to decrease the rate of visual loss and stabilize the retinal lesion. In order to obtain stabilization of the retinal lesion, Visudyne® Therapy is generally repeated multiple times on the same eye over the ensuing years.
Patients who receive Visudyne® will become temporarily photo sensitive after the infusion and are to avoid direct sunlight for 5 days. During that period, you should avoid exposure of unprotected skin, eyes or other body organs to direct sunlight or bright indoor light. This includes, but is not limited to tanning salons, bright halogen lighting, and high power lighting used in surgical operating rooms or dental offices. If you must go outdoors in daylight during the first 5 days after treatment, you should protect all parts of your skin and eyes by wearing protective clothing and dark sunglasses. UV sun-screens are not effective in protecting against photosensitivity reactions. There is no need to stay in the “dark,”and it is encouraged that you expose your skin to ambient indoor light. This will help inactivate the drug in the skin through a process called photo bleaching. Failure to comply with the above recommendation scan lead to serious injury including skin burns.
Pars Plana Vitrectomy
Vitrectomy is a surgical procedure undertaken by a Retina specialist where the vitreous humor gel that fills the eye cavity is removed to provide better access to the retina. This allows for a variety of repairs, including the removal of scar tissue, laser repair of retinal detachments and treatment of macular holes. Once surgery is complete, saline, a gas or air bubble or silicone oil may be injected into the vitreous gel to help hold the retina in position. Many vitrectomy procedures can now be performed with self-sealing, sutureless (nostitch) incisions with a micro-cannular system of approximately one half of a millimeter in size.
This procedure is almost always performed under local anesthesia in an outpatient surgery center. The eye is prepared with antiseptic solution and a sterile drape is applied. An eyelid speculum is used to keep the operative eye open. The other eye is covered and protected. Patients generally close their non-operative eye and rest during the surgery.
A surgical microscope with a special lens allows a wide view of the inside of the eye as well as a magnified and detailed view. The surgeon uses a vitrectomy probe (vitrector) and a light pipe to cut and delicately remove the gel-like vitreous. During vitrectomy surgery, the vitreous is removed via three microscopic openings in the sclera (the white part of the eye).
Several microscopic instruments may be used during the Vitrectomy, these may include forceps, scissors, and silicone tipped cannulas. In many cases endolaser is used at the end to seal retinal tears or abnormal blood vessels.
The eye is left filled with air or with a vitreous substitute such as a gas bubble or silicone oil. When a vitreous substitute is used, a period of post-operative positioning (typically face-down) by the patient helps the retina heal.Complications of surgery are rare, but include infection, bleeding, high or low eye pressure, cataract, retinal detachment, epiretinal membrane formation, and loss of vision.
When is a Vitrectomy Recommended?
The most common indications for performing a vitrectomy are:
1. Vision-affecting vitreous opacities such as Vitreous Hemorrhage or Asteroid Hyalosis
2. Conditions caused by abnormal pulling/traction on the retina such as Macular Holes, Macular Pucker, Traction Retinal Detachments, Rhegmatogenous Retinal Detachments
3. Conditions such as retained cataract fragments, intraocular foreign bodies, ordis located intraocular lenses
4. To diagnose/biopsy a vitreoretinal condition (diagnostic vitrectomy)
5.When placing a therapeutic device or drug delivery.
Treatment consists of vitrectomy to remove vitreous opacities (clouding), separation of the vitreous from the retina, membrane peeling to remove retinal traction, and placement of a gas bubble or laser as needed to prevent re-bleeding or re-detachments. Removing membranes or scar tissue from the surface of the retina is delicate and exacting work, requiring many techniques in addition to vitrectomy. Sometimes in eyes with more severe retinal detachments, vitrectomy is combined with scleral buckling, a procedure involving sewing a piece of silicone sponge, rubber, or semi-hard plastic onto the sclera or placing a band encircling the eye to relieve retinal traction.
What to expect after surgery:
The eye is generally comfortable, patched, and shielded to protect from injury. If a gas bubble or silicone oil has been used to treat the eye, your surgeon will give you instructions on how to do any required positioning (such as face-down), and how long you should continue it.The gas bubble serves to press the retina back into its normal position and hold it there until the eye heals. You will need a driver because you will be sedated and driving is prohibited. When you return to the doctor’s office one day after surgery, it is advisable to have a driver to assist until your sight has returned enough to drive yourself. If a gas bubble has been used, air travel, use of nitrous gas anesthesia, and ascending to higher altitudes should be strictly avoided to reduce the risk of elevated eye pressure. Your doctor will give specific instructions on when you may resume these activities. Maintaining head and eye positioning after a vitrectomy involving a gas bubble or silicon oil is a very important way to contribute to the success of your eye surgery.
On your first post-operative visit, your doctor and her or his staff will review instructions for medications, drops, positioning, use of the eye patch, and general activities. You will also schedule your next follow-up appointment. You should NOT drive until you feel fully safe and capable of operating your vehicle; this can vary from a few days to several weeks following surgery.
Recovery:
After the Vitrectomy, the saline solution or gas bubble is gradually replaced by the eye’s own fluids (the aqueous humor). The gas bubble typically lasts for 6 weeks inside the eye and will slowly reabsorb. A horizontal line will be seen as the gas bubble diminishes. If silicone oil is used as a vitreous substitute to help more serious conditions heal, a second procedure may be performed several months after surgery to remove the silicone oil. There may be some temporary swelling of the eyelids, hemorrhages around the eye, and redness following the surgery, but these improve relatively quickly.
A mild sensation as if there is something in your eye is common following surgery, specially if sutures are required, but severe pain is uncommon unless there is unusual inflammation or high eye pressure. You will be prescribed several eye drops, usually antiriotics and anti-inflammatory in nature which are very important to help the eye heal.
Some patients will note a decrease in vision for a few days following the procedure.Others, particularly if a gas bubble or silicone oil is used, may need weeks or even months for the vision to improve.
Safety and Results:
Severe complications are rare and anatomic success for vitrectomy is over 90% for many conditions. Advances in instrumentation, techniques, and understanding of diseases of the vitreous and retina have made vitrectomy and retina surgery more successful.
Scleral Buckle Surgery
Scleral Buckle Surgery is a long-established technique used to repair a retinal detachment. Scleral buckles may be performed for inferior retinal detachments or in combination with Pars Plana Vitrectomy for more severe retinal detachments. This surgery is outpatient and performed under local anesthesia. It is a method of closing breaks and flattening the retina. A small, invisible synthetic band, usually made of silicone rubber, is attached to the outside of the eyeball to gently push the wall of the eye against the detached retina. This relieves the traction caused by retinal breaks and also displaces some retinal fluid away from the break. Different sizes and types of scleral buckles may be used, depending on the nature of the detachment. Cryotherapy and/or Laser may be used to treat associated retinal tears. Scleral buckles are usually left on the eye permanently. Single operation success rates for scleral buckle are generally high.
A common side effect of scleral buckle surgery is increased near sightedness. There are many less common complications that include eye infection, increased eye pressure, bleeding, injury to other parts of the eye, cataract, droopy eyelid and double vision.
Complete vision loss is very rare, but still possible as a result of scleral buckle surgery. Since this procedure can change the shape of the eye, you will need to have your contact lens or glasses prescription checked, and probably changed. If the initial operation is unsuccessful, additional surgery is likely to be recommended.

Icons & Graphics
Icons and other Graphics were manually designed by the BRIX Elements team. You may download these and edit them to fit your website without asking for permission or providing credit.
Upon purchasing Medica team, our team grants you a nonexclusive, worldwide copyright license to download, copy, modify, and use the icons.
Photography
All images used in the Medica Webflow Template are licensed for free personal and commercial use.
If you'd like to use any specific image, can can check the licenses and download the images for free on Unsplash, Pexels, Burst, and Freepik.
The licenses are break down below:
Unsplash: Image 1, Image 2, Image 3
Pexels: Image 1, Image 2
Burst: Image 1
FreePik: Image 1, Image 2, Image 3, Image 4, Image 5, Image 6